
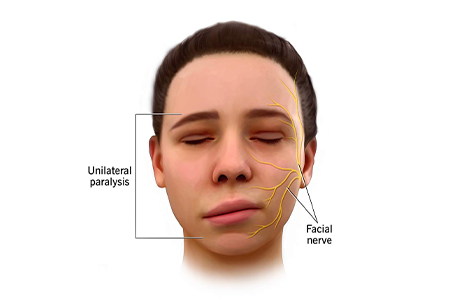
Facial Palsy
Facial palsy is caused by damage to the facial nerve (i.e. cranial nerve VII) that supplies the muscles of the face. It can be categorised into two types based on the location of the casual pathology:
- Central facial palsy – Due to damage above the facial nucleus
- Peripheral facial palsy – Due to damage at or below the facial nucleus
Cause :
Upper motor neurone causes:
- Stroke
- Intracranial tumour
- Multiple sclerosis
- Syphilis
- HIV
- Vasculitides
- Haemorrhage
Lower motor neurone causes
- Idiopathic or Bell’s Palsy
Common Cause :
Its cause is not known, but it is likely linked to Herpes Simplex infection.
- Tumour
A tumour compressing the facial nerve can cause facial paralysis, but more commonly the facial nerve is damaged during surgical removal of a tumour. The most common tumour to cause facial palsy during surgical removal is the acoustic neuroma (also known as vestibular schwannoma).
Less common tumours to cause facial palsy (or the surgery to remove them) include cholesteatoma, hemangioma, facial schwannoma or parotid gland tumours.
- Infection
Ramsay Hunt syndrome – caused by Herpes Zoster infection. This is a syndromic occurrence of facial paralysis, herpetiform vesicular eruptions, and vestibulocochlear dysfunction. Patients presenting with Ramsay Hunt syndrome are generally at increased increased risk of hearing loss than patients with Bell’s palsy, and the course of disease is frequently more painful. There is also a lower recovery rate from facial palsy in Ramsay Hunt syndrome patients
Lyme disease – caused by infection with Borrelia burgdorferi via tick bites. Around 10 percent of patients affected with lyme disease develop facial paralysis – 25 percent of these patients present with bilateral facial palsy
- Iatrogenic facial nerve damage – Occurs most commonly in temporomandibular joint replacement, mastoidectomy and parotidectomy
- Trauma – Especially temporal and mastoid bone fractures
- Congenital – A very small number of babies are born with congenital dysfunction of the facial nerve
Rare causes :
- Neurosarcoidosis
- Otitis media
- Multiple sclerosis
- Moebius syndrome
- Melkersson-Rosenthal syndrome
- Guillain-Barre syndrome
- Millard-Gubler syndrome (AKA ventral pontine syndrome)
- An ipsilateral facial palsy with contralateral hemiplegia that involves the corticospinal tract and paralysis of lateral rectus on the ipsilateral side due to the involvement of the abducent nerve
- Foville Syndrome (AKA inferior medial pontine syndrome)
- An ipsilateral facial palsy, contralateral hemiplegia with ipsilateral conjugate gaze effects
- Eight-and-a-half syndrome
- Facial palsy with internuclear ophthalmoplegia and horizontal gaze palsy
Symptoms :
Appearance and Range of Movement
- Inability to close the eye
- Inability to move the lips (e.g. into a smile, pucker)
- At rest, the affected side of the face may “droop”
- If, however, the person is in synkinesis, the affected side of the mouth may sit higher than the unaffected side. Facial synkinesis is defined as “abnormal facial movements that occur during volitional or spontaneous movement, for example, voluntary movement of the mouth may result in the closure of the eye”
- Ectropion – i.e. the lower eyelid may droop and turn outward
Functional Effects
- Difficulty eating and drinking as the lack of lip seal makes it difficult to keep fluids and food in the oral cavity
- Reduced clarity of speech as the “labial consonants” (i.e. b, p, m, v, f) all require lip seal
- Dryness of the affected eye – more information on this is available here
Somatic Effects
The facial nerve supplies the lachrymal glands of the eye, the saliva glands, and to the muscle of the stirrup bone in the middle ear (the stapes). It also transmits taste from the anterior two thirds of the tongue.
Facial palsy often involves:
- Lack of tear production in the affected eye, causing a dry eye, and the risk of corneal ulceration
- There are two factors which contribute to dry eye in facial nerve palsy:
- The greater petrosal nerve, derived from the facial nerve, is affected – it supplies the parasympathetic autonomic component of the lacrimal gland, controlling the production of moisture / tearing in eyes.
- The zygomatic branch of the facial nerve supplies orbicularis oculi, and the resulting paralysis leads to an inability (or reduced ability) to close the eye or blink. Thus, tears (or artificial lubrication in the form of drops, gel, or ointment) are not spread across the cornea properly.
- Hyperacusis – i.e. sensitivity to sudden loud noises
- Altered taste sensation
Treatments :
- Nasyam
- Shirovasthi
- Shirodhara
- Abhyanga
- Mridu swedana
- Nadi balya
- Brmhana
- Dravya prayoga
- Snigdha-Amla-and Lavana rasa prayoga and Vatahara oushadha (Vata balancing medicine and treatment)
- Tharpana
- Shiro Pichu
- Mukhabhyanga
- Panasa Patra Sweda
- Gandusha
- Kavala
- Karna poorana
- Thala
- Ksheeradhara
- Pichu
- Shirovasti
- Ksheeradhooma
- Lepana
- Rehabilitation therapy